Brain fog is the everyday description for a state most people have lived inside more than once: thinking feels slow, the right word does not come, holding two things in mind at the same time is too expensive to attempt, and tasks that ordinarily take fifteen minutes take an hour or do not finish. The word feels imprecise, and it is. Brain fog is not a diagnosis, not an ICD-10 code, not a neurological entity in any textbook. It is a description that survived because the underlying experience is so common: a global slowdown of the cognitive control system that gives you no clear other label.
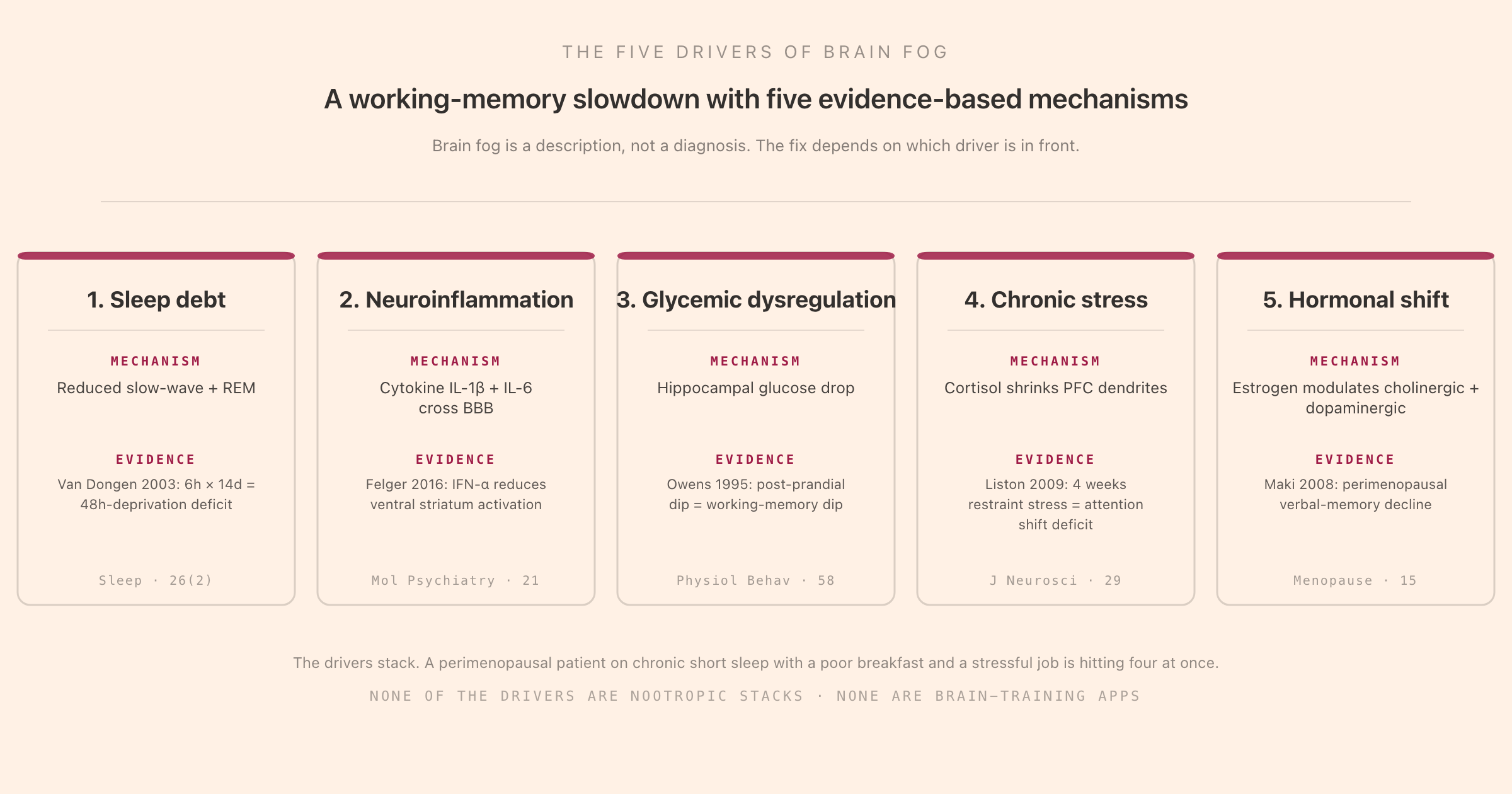
This piece is the cognitive-science version of brain fog. The argument is that brain fog is a working-memory and executive-function slowdown, with five evidence-based drivers (chronic sleep debt, neuroinflammation, glycemic dysregulation, chronic stress, and hormonal shift) that each lower the throughput of the same system in slightly different ways. The fix is rarely more effort. The fix is identifying which driver is in front and removing it. Tomatoes is a focus tool built around making the working block itself cheaper to hold (steady audio masks variable environmental sound, the timer externalises goal-holding, the cycle removes the shifting decision). It cannot fix sleep debt or perimenopausal estrogen withdrawal. It can make the difference between "I can still get something done while the driver is being worked on" and "I cannot work at all today." The app is a one-time $39 with no subscription.
What Brain Fog Actually Is
Brain fog is a description, not a disease. The phrase has clinical purchase only in a few specific contexts (post-COVID neurocognitive symptoms, chemo-brain in cancer patients, fibromyalgia "fibro fog," and chronic-fatigue-syndrome cognitive complaints), and in those contexts the symptom cluster is consistent enough to be measured. Outside those contexts, the term covers a wider population of people who describe a recurrent or sustained slowdown of mental performance without obvious cause. The neuropsychology literature treats it as a transdiagnostic complaint that maps onto a specific cognitive profile: reduced working-memory throughput, slowed processing speed, impaired attentional control, and reduced subjective alertness.
Three properties of the experience that the science of working memory and executive function help clarify:
Brain fog is a throughput problem, not a knowledge problem. Crystallised knowledge stays intact. Vocabulary, expertise, autobiographical memory, procedural skill, all the things that survived the night before survive the foggy morning too. What collapses is the ability to bring them together fast enough to do work. The vocabulary is there; the access is slow. The plan is there; constructing the next step is effortful.
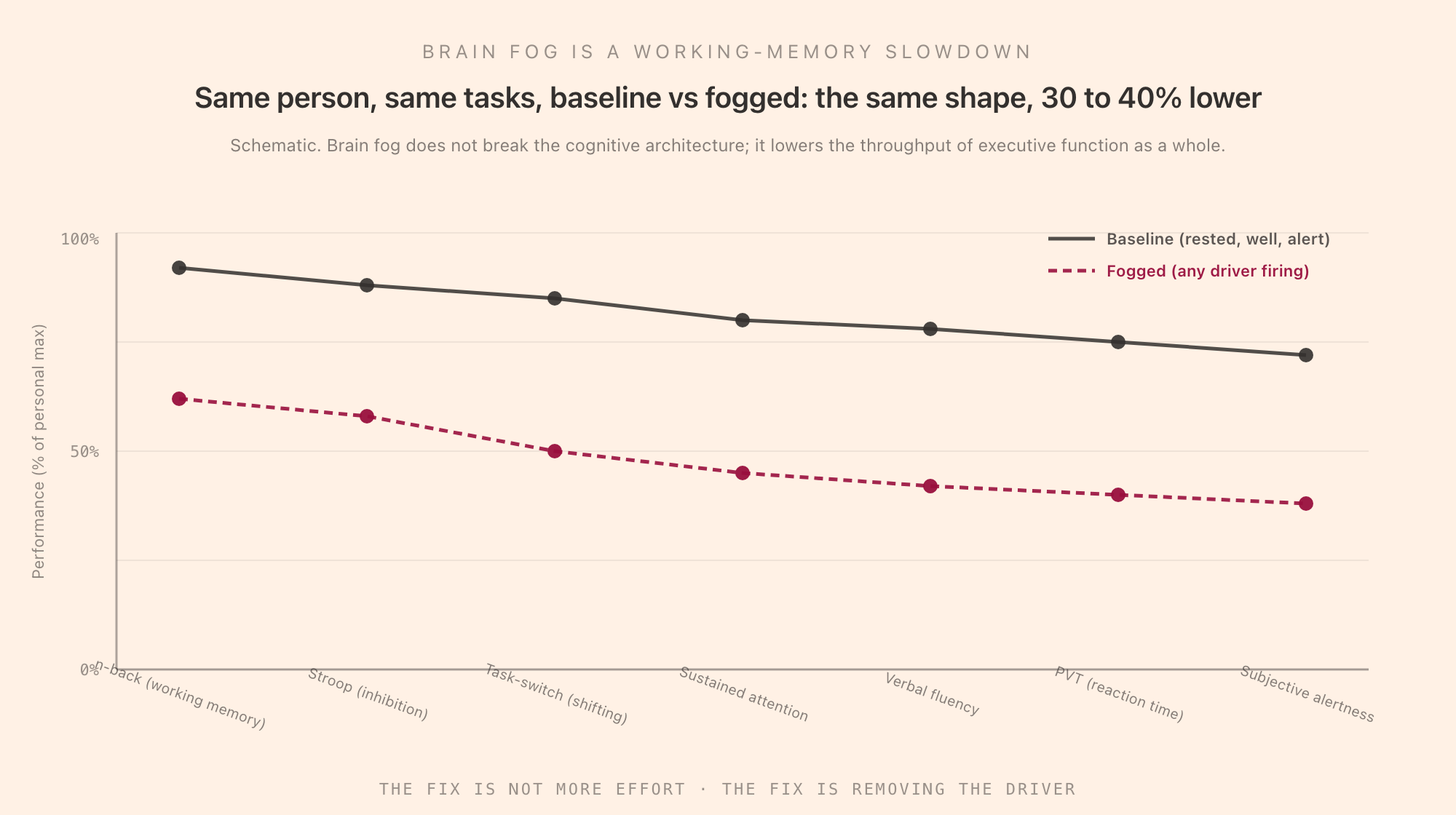
The slowdown is the same shape, just lower. People describe brain fog in different vocabulary depending on what cognitive task they were just trying to do, but the underlying impairment is broadly uniform: working memory, inhibition, shifting, sustained attention, and reaction time all go down together. This is what the executive-function literature would predict, because the common factor underneath these tasks (Miyake's "common executive component") is exactly what the drivers below are lowering.
Subjective effort goes up while objective output goes down. This is the signature mismatch of cognitive depletion. Foggy work feels harder per minute and produces less per hour. The hours-of-effort intuition that ordinarily predicts output stops being a reliable signal.
The Five Drivers
The mechanistic literature on cognitive slowdown converges on five major drivers. They overlap, they stack, and a person hitting two or three at once is in a different functional state than a person hitting one. The five:
1. Chronic Sleep Debt
The most common, the most under-rated, and the cheapest to fix in principle. Sleep debt is the chronic mismatch between the sleep the brain needs (roughly seven to nine hours for adults, with individual variation but a narrow distribution) and the sleep it gets. The canonical evidence is Van Dongen and colleagues (2003), who ran adults on four, six, or eight hours per night for fourteen days and measured cognitive performance daily. The six-hour group's performance on the Psychomotor Vigilance Task at day 14 was indistinguishable from that of subjects who had been kept awake for forty-eight straight hours, while the participants themselves rated their subjective alertness as only mildly impaired. This is the most-cited evidence that subjective alertness is not a reliable proxy for objective cognitive performance under chronic short sleep.
The mechanism is not single. Slow-wave sleep is reduced first; SWS supports overnight memory consolidation and clearance of metabolic waste from the brain through the glymphatic system. REM sleep is reduced second; REM supports emotional regulation and certain forms of procedural learning. Beyond about a week of restriction, the prefrontal cortex shows measurable hypofunction on neuroimaging, which lines up exactly with the working-memory and inhibition deficits the cognitive testing finds. The circadian rhythm piece covers the timing-side companion to total sleep time; brain fog from circadian misalignment looks the same as brain fog from short sleep because the underlying mechanism overlaps.
2. Neuroinflammation
Brain fog became a household word during the post-COVID era specifically because long-COVID brain fog gave a name to the cognitive consequence of systemic inflammation. The mechanism: peripheral inflammation (from infection, autoimmune flare, metabolic disease, even chronic poor sleep, which is itself proinflammatory) produces elevated cytokines, especially interleukin-1 beta (IL-1β), interleukin-6 (IL-6), and tumour necrosis factor alpha (TNF-α), some of which cross the blood-brain barrier and others of which signal across it via the vagus nerve and circumventricular organs. The brain responds with microglial activation, altered neurotransmission, and reduced regional activity in reward and motivation circuits.
The cleanest experimental work comes from interferon-alpha studies in hepatitis C patients (Capuron, Felger, Miller and colleagues), where giving IFN-α as a treatment for hepatitis induced depression-and-fatigue symptoms in roughly a third of patients, complete with measurable reductions in ventral striatum activation and dopamine signalling. The model that emerged is that the cytokines downregulate dopaminergic function in the reward circuit, which is read clinically as anhedonia and fatigue, and cognitively as slowed processing and impaired motivation. The same circuit produces the "I can't be bothered to start" half of brain fog.
Long-COVID brain fog appears to be the same picture from a different trigger: persistent low-grade neuroinflammation, sometimes accompanied by microvascular changes, producing the same cytokine-mediated downstream effects. The persistence beyond the acute infection is the part that is still being characterised, but the mechanism family is consistent with what was already known.
3. Glycemic Dysregulation
The brain uses about 20% of the body's glucose at rest. Sharp swings in blood glucose, both spikes and the rebound dips that follow them, produce measurable cognitive effects. The Owens and colleagues 1995 study is one of the earliest careful demonstrations: testing working memory and attention across post-prandial windows in healthy subjects, the post-prandial dip in glucose (roughly 90 to 180 minutes after a high-glycemic-index meal) produced reliable decrements on working-memory tasks, with subjects reporting subjective fogginess that tracked the dip. Subsequent work has replicated and extended this in both healthy and diabetic populations.
The hippocampus is particularly sensitive to glycemic state because it has high metabolic demand and is one of the regions affected by glucocorticoid-stress crosstalk (see driver 4 below). A breakfast of refined carbohydrate followed by a 10:30am slump is a tightly mechanistic experience; the brain is running on a glucose curve that rises fast, falls fast, and leaves the prefrontal-and-hippocampal system briefly under-supplied. The intervention literature here is straightforward: meals with a lower glycemic load, protein at breakfast, and avoiding long fasts in people whose glycemic control is borderline. None of which is exotic; all of which works.
4. Chronic Stress
Acute stress sharpens cognition for short windows. Chronic stress does the opposite, and the chronicity itself is the variable that matters. The Liston, McEwen, and Casey 2009 paper in the Journal of Neuroscience demonstrated this in humans by comparing medical students at high-stress points in their training to themselves at lower-stress baseline: the high-stress condition produced measurably impaired attention-shifting performance and a corresponding reduction in dorsolateral prefrontal cortex activation on fMRI. McEwen's broader research programme on allostatic load showed that chronic glucocorticoid elevation produces dendritic shortening in the prefrontal cortex and dendritic hypertrophy in the amygdala, a pattern that biases the brain toward threat detection and away from goal-directed control. Read functionally: chronic stress shrinks the part of the brain that does executive work and grows the part that interrupts it.
The cognitive signature of chronic stress is brain fog plus irritability plus rumination, with the rumination piece functioning through the default mode network becoming sticky (harder to suspend during goal-directed work). The interventions with the strongest evidence are physical exercise, sleep, social support, and the structured stress-reduction protocols (MBSR, CBT, behavioural activation), all of which reduce baseline cortisol and reverse the allostatic-load picture over weeks to months.
5. Hormonal Shift
Perimenopause produces some of the cleanest documented cases of objectively measurable brain fog. Maki and colleagues' 2008 work in Menopause and the broader Study of Women's Health Across the Nation (SWAN) cohort have shown that the menopause transition is associated with verbal memory decline that is detectable on standardised cognitive testing, with the strongest signal during the perimenopause itself rather than after the post-menopause stabilisation. The mechanism involves estrogen's role in modulating both cholinergic and dopaminergic systems, plus its direct effects on hippocampal neurogenesis and synaptic plasticity. The decline is real, it tracks the hormonal trajectory, and it is largely transient: the cognitive picture stabilises and partially recovers after menopause is established.
Other hormonal contributors: thyroid dysfunction (both hypo- and hyper-, both produce cognitive slowing, and screening with TSH is one of the cheapest brain-fog work-ups available), pregnancy (the "pregnancy brain" experience is supported by neuroimaging evidence of regional grey-matter changes during gestation), and the post-partum period. The testosterone literature in older men is more mixed; effects on cognition appear smaller than the menopause literature.
The five drivers are not in competition. A perimenopausal patient on chronic short sleep with a high-glycemic breakfast and a stressful job is hitting four drivers simultaneously, and the resulting brain fog is more than additive because each driver makes the others worse (sleep loss is proinflammatory, inflammation worsens insulin sensitivity, stress disrupts sleep, glycemic crashes elevate cortisol).
How to Get Rid of Brain Fog: What Has RCT Evidence
The interventions that have actual randomised-controlled-trial evidence for cognitive improvement in brain-fog-like populations are not exotic. Sorted roughly by effect size and reliability:
Sleep restoration. The single highest-leverage intervention, because chronic short sleep is the most common driver and because the dose-response curve is steep. Going from six to seven and a half hours of nightly sleep produces measurable cognitive improvements within two weeks for most people. The intervention is not always trivial (sleep onset insomnia, sleep maintenance insomnia, sleep apnoea, and circadian misalignment all need different approaches), but the upper bound on the improvement is large. CBT-I (cognitive-behavioural therapy for insomnia) has the strongest evidence base for insomnia-driven sleep restriction.
Physical exercise. Aerobic exercise has been studied repeatedly in older-adult cognitive-decline populations and in younger working-age populations with subjective cognitive complaints. Meta-analyses converge on effect sizes in the small-to-medium range (Cohen's d around 0.2 to 0.4) across executive function, attention, and processing speed. The mechanism is multiple: improved cerebral blood flow, increased BDNF (brain-derived neurotrophic factor), improved insulin sensitivity, improved sleep, reduced inflammation, reduced cortisol. The minimum effective dose appears to be roughly 150 minutes per week of moderate aerobic activity. The effects show up within four to twelve weeks of consistent training.
Time-restricted eating, when glycemic dysregulation is in play. The intervention here is to compress the eating window to roughly eight to twelve hours during the day, eat lower-glycemic-load meals, prioritise protein at breakfast, and avoid late-evening eating. The benefits are partly glycemic and partly circadian (eating late shifts peripheral clocks out of phase with the central clock). For people with insulin resistance or pre-diabetic glycemic markers, the cognitive benefits track the improved glucose curves.
Light therapy and morning bright light. Particularly useful when circadian misalignment or seasonal affective contribution is part of the picture. Twenty to thirty minutes of bright light within the first hour after waking advances and stabilises the circadian phase, which improves sleep timing, which feeds back into the sleep-restoration leverage above.
Working-memory training for some narrow uses. The Melby-Lervåg and colleagues meta-analyses showed that working-memory training reliably improves performance on the trained task and on closely related near-transfer tasks, but does not transfer to general cognitive ability or to everyday function. The implication for brain fog: training does not "lift the fog" in any general sense, but it can improve performance on a specific task that is degraded by working-memory load if you are willing to drill that task. The benefits are narrow.
Mindfulness-based stress reduction (MBSR) for the stress driver. Kabat-Zinn-derived structured programmes have evidence for reducing perceived stress and improving sustained-attention performance. The effect sizes are modest and the requirement is consistency (the studies typically use 8-week protocols with daily practice), but the intervention is real and the side-effect profile is benign.
Hormone replacement therapy for the perimenopausal driver, in selected patients. The cognitive evidence for HRT in perimenopause is mixed but has improved with newer transdermal and bioidentical formulations and with treating earlier in the menopause transition rather than after. This is a clinical conversation, not a self-administered intervention, but the cognitive benefit is one of the explicit reasons it has come back into mainstream practice after the WHI-era retreat.
Treating the medical condition driving the inflammation. When neuroinflammation is the driver, the path forward is upstream: managing the autoimmune disease, treating the chronic infection, addressing the metabolic syndrome, treating the sleep apnoea. There is no intervention that "cures" generalised neuroinflammation; the cognitive benefits track the resolution of the underlying inflammatory process.
Three Interventions That Do Not Work
The brain-fog supplement market is large, profitable, and mostly unsupported. Three categories worth ignoring:
Generic nootropic stacks. The combinations of vitamins, herbs, and "smart drugs" marketed for cognitive enhancement have, with a few specific exceptions, no high-quality evidence for benefit in healthy adults. Caffeine works for short-term alertness and is the only universally established cognitive enhancer in this category. L-theanine pairs with caffeine to reduce the jittery side effect with some supportive evidence. Modafinil (prescription only) has narrow evidence for sleep-deprived performance. Most other ingredients in nootropic blends have either no evidence or evidence too thin to act on.
"Brain-training" apps that promise transfer. The Owen, Bavelier, and broader literature on commercial brain-training apps consistently finds that the trained task improves and the transfer to general cognition is at best minimal. Lumosity paid $2 million to the FTC in 2016 to settle claims about exaggerated cognitive benefits. Newer products make narrower claims, but the underlying transfer problem is the same: drilling a working-memory task improves that task and a few close cousins, not your general cognitive throughput.
Detox protocols. Liver detoxes, lymphatic detoxes, parasite cleanses, and the broader "remove the toxins" framing have no mechanistic relationship to brain fog as documented by the cognitive-science literature. The body has well-characterised detoxification systems (liver, kidneys); they do not require external supplementation in healthy adults; and the cognitive complaints of the people who feel better after a "detox" are nearly always responding to the incidental changes (better sleep, reduced alcohol, better hydration, less ultra-processed food) rather than the detox itself.
Brain Fog in ADHD and Long-COVID: Two Special Cases
ADHD itself is not "brain fog," but the cognitive profile of unmedicated or under-supported ADHD produces a brain-fog-like presentation, particularly when the patient is on chronic short sleep or unmedicated. The mechanism is somewhat different: ADHD is a structural pattern of executive-function impairment (Russell Barkley's reframe of ADHD as a working-memory disorder is the cleanest statement of this) with a strong genetic basis, rather than an acute state. The interventions that work for ADHD (medication, behavioural scaffolding, structure) overlap incompletely with the interventions that work for brain fog from the drivers above. The ADHD and focus music piece covers the audio-side intervention; the executive-function piece covers the broader pattern.
Long-COVID brain fog has been documented well enough to have its own clinical literature now. The cognitive profile maps onto the neuroinflammation driver from section 2, with persistent symptoms ranging from weeks to months to (in a smaller subset) years. Standardised cognitive testing in long-COVID patients shows real, measurable deficits, often disproportionate to the patients' self-rated severity. Recovery is the rule but not universal, and the time course is highly variable. The interventions that have shown benefit are largely the general brain-fog interventions above (sleep, exercise titrated against post-exertional malaise, stress management, treating co-morbid sleep apnoea or anxiety) plus the specific long-COVID protocols that some specialist clinics have developed. There is no single magic intervention.
What This Means for Daily Focus Work
The model has three practical implications for daily focus work.
Identify the driver before reaching for tactics. A focus app cannot fix sleep debt, perimenopausal hormonal flux, or untreated sleep apnoea. The first question with persistent brain fog is which driver is in front, because the intervention is driver-specific. Working-memory training, brain-training apps, and meditation do not substitute for actually sleeping seven and a half hours.
Externalise as much of the executive load as the driver lets you. Lists, timers, calendar reminders, single-purpose work environments, and pre-decided "what I will work on next" are all ways to move executive load out of the prefrontal cortex (which the drivers have weakened) and into the environment (which they have not). The lower your throughput, the more leverage offloading has. The pomodoro technique piece covers the timer pattern specifically.
Reduce the inhibition cost of the environment. Inhibition is one of the three Miyake components and is the cheapest to spend without realising you have spent it. Open browser tabs, notification badges, a variable acoustic environment, and visible clutter each carry an inhibition tax. Removing them is cheaper than suppressing them. Steady audio, monochannel acoustic environment, and visible-screen minimalism are all interventions in this category. A focus-audio channel does not lift the fog. It does lower the inhibition bill the fogged executive system is paying, so the impaired executive budget goes further.
The cognitive load piece and executive function piece cover the architecture this section assumes; the circadian rhythm piece covers the timing-side companion to total sleep time; the procrastination piece covers the motivation-side overlap.
The Bottom Line
Brain fog is a description of a working-memory and executive-function slowdown that survives because the experience is universal and the underlying state is real. It is not a diagnosis. It is the cognitive consequence of five major drivers, sleep debt, neuroinflammation, glycemic dysregulation, chronic stress, and hormonal shift, and a person feeling foggy is almost always hitting at least one and often more than one. The interventions that work are unglamorous: sleeping more, exercising, eating in a way that does not crash blood sugar, managing stress, and treating the medical conditions that drive inflammation. The interventions that do not work are the ones the supplement industry sells. Brain-training apps and detox protocols cannot replace the seven and a half hours.
The role of a focus tool inside this picture is narrow but real. The drivers cannot be fixed by software. But the executive system the drivers have weakened still has to do work today, and the cheapest way to support it is to give it less to fight. A steady audio channel that masks the variable environmental sound, a timer that holds the goal, and a fixed block that removes the shifting decision are all interventions on the inhibition and shifting side of the Miyake model. Tomatoes is built around that pattern and is a one-time $39 with no subscription. The fog comes from elsewhere; the work still has to happen.